 Figure
1
Figure
1Cassandra B.
Fremder
Abstract
The objective of this experiment was to determine if gender
or self-esteem contributed to the development of eating disorders. The study
involved a total of 100 students who participated by completing a survey used to
examine self-esteem, dietary habits, and experience with eating disorders.
Results found that participants who reported higher self-esteem also reported
less experience with eating disorders. Additionally, it was found that females
rated themselves lower for self-esteem and were more likely to report experience
with an eating disorder than did males. These results indicated a significant
correlation between self-worth and eating disorders, as well as a significant
correlation between gender and self-esteem, and gender and eating disorders.
Therefore, it can be said that both hypotheses were supported within this
sample, suggesting that students with high self-esteem are less likely to have
an eating disorder, and that women are more likely than men to suffer from
eating disorders.
Self-esteem is an important issue in eating disorders. It has been known
that gender, self-esteem, body image, and perceived self-worth seems to be
related to dietary habits and eating disorders; but researchers have wanted to
understand the relationship more clearly, comprehending the degrees to which
they interact with each other. Many research studies have presented the idea
that those who suffer from an eating disorder are more likely to have lower
self-esteem than those who do not have an eating disorder (e.g. de la Rie,
Noordenbos, & Furth, 2005; Hesse-Biber, Marino, Watts-Roy, 1999). These studies
and others have shown that eating disorders are associated with lower levels of
self-esteem and perception of self-concept. Additionally, research regarding the
impact of gender on self-esteem has continually supported the idea that women
are more likely than men to report lower levels of self-esteem and endorse
eating disorders (e.g. Green, Scott, Cross, Liao, Hallengren, Davids, & Jepson,
2009). Although much research has been conducted to show the degrees of relation
between self-esteem, gender, and eating disorders among various populations, few
studies have attempted to find these correlations among college students. The
motivation that prompted this research study was to determine if students with
higher self-esteem were less likely to develop eating disorders and to
understand the impact of gender on self-esteem and eating pathology.
For example, de la Rie, Noordenbos, and Furth (2005) sought to measure
the quality of life of eating disorder patients and former eating disorder
patients. The purpose of this study was to investigate whether the quality of
life differs between four diagnostic groups: anorexia nervosa patients, bulimia
nervosa patients, eating disorder not otherwise specified patients and former
eating disorder patients, and to understand what factors influence the quality
of life. To do this, the experimenters administered a generic health-related
quality of life questionnaire, the Short Form-36, and the Eating Disorder
Examination-Questionnaire to 156 eating disorder patients (44 anorexia nervosa
patients, 43 bulimia nervosa patients, 69 eating disorder not otherwise
specified patients) and 148 former eating disorder patients, all recruited from
different parts of the Netherlands by various means. A limitation of this study
was that participants were not asked to report on whether or not they had
comorbid disorders. Another limitation was that the advertisements to
participate in this study may have appealed especially to those who have
received treatment for eating disorders.
The results of the de la Rie, Noordenbos, and Furth (2005) study
indicated that eating disorder patients had significantly poorer quality of life
measures than the former eating disorder patients on the Short Form-36 subscales
of Physical Role Functioning, Emotional Role Functioning, Vitality, General
Health Perception, Social Functioning and Mental Health. Additionally, no
significant differences were revealed between eating disorder diagnostic groups
with regard to the quality of life, except on General Health Perception.
Anorexia nervosa and eating disorder not otherwise specified patients reported
poorer quality of life than former eating disorder patients on General Health
Perception, but not bulimia nervosa patients. Higher self-esteem was associated
with a higher score on General Health Perception and with a higher score on
vitality. These findings presented that self-esteem showed the highest
association with the quality of life of both eating disorder patients and former
eating disorder patients.
Previous studies have sought to observe to correlations of self-worth and
eating disorders. On the contrary though, not many have researched these in
regard to college students. Hesse-Biber, Marino and Watts-Roy (1999) conducted a
longitudinal study to determine whether women in the college population who
suffered from eating disorders during their college years would recover during
their post-college years. The participants, who included 144 women in the
original population, were asked to answer questionnaires during their sophomore
and senior years of college. Later, the twenty-one participants that continued
for the duration of the six-year study were engaged in in-depth interviews that
covered a wide range of psychological, environmental, developmental, and
sociocultural factors. A limitation of this study was that the researchers
relied on qualitative data rather than hypothesis testing and replication of
past studies.
After the interview, participants
answered a short questionnaire, which dictated demographic information and used
continuum scales to measure eating patterns. The Eating Habits Scale consists of
five categories: normal eaters, normal dieters, presyndrome, at risk and problem
eaters. Women in the study were placed in these categories during three
different points in time: sophomore year, senior year, and two years
post-graduation. The Changes in Eating Habits Scale measured changes in
individual eating patterns from the sophomore year to the senior year and from
the senior year to two years post-graduation. It was designed to capture the
ways in which eating patterns could change. The researchers (Hesse-Biber, et
al., 1999) found that eleven women �got better�: that their disrupted eating
patterns in college returned to normal post-graduation, and that ten women
�remain at risk�: that they continue to exhibit tendencies toward disordered
eating and distorted body image. A pattern of healthy self-concept emerged for
the eleven women in the �got better� group; themes of their interviews were
confidence, autonomy, success in job and success in relationships. For those
that remain at risk, their relationships are described as tense, dissatisfaction
was reported in the autonomous realm, and the women expressed self-doubt and a
diminished self-esteem.
Another study (Green, Scott, Cross, Liao, Hallengren, Davids, Carter,
Kugler, Read, & Jepson, 2009) examined whether a unique relationship exists
between depression and eating disorder behaviors after controlling for
maladaptive social comparison, body dissatisfaction, and low self-esteem. The
participants were a volunteer sample with a total of 208 participants, with ages
ranged from seventeen to thirty-two years and body weights ranged from ninety to
345 pounds. Participants included 127 undergraduate women and eighty-one
undergraduate men who completed a demographic questionnaire, the Eating Disorder
Examination-Questionnaire, the Rosenberg Self-Esteem Scale, the Body Shape
Questionnaire � Shortened Version, the Social Comparison Rating Scale, and the
Beck Depression Inventory-II. The results indicated that undergraduate women
were more likely to endorse eating disorder pathology. Additionally, the
hypothesis was supported, that minimal unique variance was found in eating
disorder behaviors explained by depression after controlling for maladaptive
social comparison, body satisfaction, and low self-esteem. A limitation of this
study was its exclusive reliance on self-report measures and failure to
incorporate biological and sociocultural predictors.
There are many steps in recovery from an eating disorder, including
biological, psychological, social, behavioral, and emotional aspects.
Additionally, research by Bardone,-Cone, Schaefer, Maldonado, Fitzsimmons,
Hamby, Lawson, Robinson, Tosh, and Smith (2010) provides support that an
improved self-concept may be an integral part of full eating disorder recovery.
In an experiment that focused on measures of self-esteem, self-efficacy and
self-directedness, these researchers hypothesized that individuals fully
recovered from an eating disorder would have higher self-esteem, self-efficacy
and self-directedness than individuals partially recovered from an eating
disorder or those currently meeting criteria for an eating disorder.
Participants included ninety-six current and former female eating disorder
patients from the University of Missouri Pediatric and Adolescent Specialty
Clinic and sixty-seven healthy control participants who were aged sixteen and
older with no current or past eating disorder symptoms.
Participants were told to fill
out questionnaires and also participated in an interview, which operationalized
eating disorders using the Structured Clinical Interview for DSM-IV, Patient
Edition, the Eating Disorders Longitudinal Interval Follow-Up Evaluation
Interview, the Eating Disorder Examination-Questionnaire, and the Body Mass
Index. Self-concept was operationalized by using the Rosenberg Self-Esteem
Scale, the General Self-Efficacy subscale of the Self-Efficacy Scale, and the
Self-Directedness subscale of the Temperament and Character Inventory. Results
indicated that the healthy controls and fully recovered group did not differ
significantly in global self-esteem, self-efficacy, or self-directedness.
Additionally, the partially recovered group was not significantly different from
the active eating disorder group, although there was a marginally significant
difference (p = .06) for intimate relationships. The nature of this study made
the experimenters able to examine self-concept variables across various stages
of an eating disorder: active, partially removed, and fully recovered.
Ross and Wade (2004) presented a study in which they investigated
mediational processes by which variables may work together to increase the
likelihood of dietary restraint and uncontrolled eating, directed by the
framework suggested by the cognitive model. The researchers� sample consisted of
111 female college students aged between eighteen and twenty-five years, as this
is likely when eating disorders develop. A self-image questionnaire was
distributed to participants, who were asked to indicate the answer which was
true for them at that particular moment in time. Their individual Body Mass
Index was also calculated. Self-esteem was assessed using the State Self-Esteem
Scale (SSES), where lower scores are indicative of lower self-esteem. Concerns
about weight and shape, dietary restraint, and uncontrolled eating were measured
using the Eating Disorders Examination-Questionnaire, where higher scores are
indicative of higher degree of restrained eating behavior, and the Eating
Disorders Inventory-2, where higher scores are indicative of a higher degree of
uncontrolled eating behavior.
Results of this study indicated that BMI, externalized self-perception
and self-esteem together accounted for 54.9 per cent of the variance in
overvalued ideas about body weight and shape, thus self-esteem partially
mediated the relationship between externalized self-perception and a combined
measure of weight and shape concern. Self-esteem and weight shape concern
together accounted for 30.2 per cent of the variance in uncontrolled eating;
therefore, weight and shape concern fully mediated the relationship between
self-esteem and uncontrolled eating. Dietary restraint did not mediate the
relationship between weight and shape concern and uncontrolled eating.
In a study conducted by Tchanturia, Troop and Katzman (2002), 245 women
from Georgia completed a number of questionnaires to determine whether weight
and shape affect self-esteem and self-worth for women of non-Western countries
as much as it affects those of Western countries. The participants were
considered an �at-risk� sample for eating disorders, including participants
engaging in psychotherapy, patients at a somatic clinic, or women in a
diet/shaping club. The questionnaires, measuring eating pathology, anxiety and
depression, as well as two measures concerning their evaluation of weight and
shape in relation to self-esteem, were distributed to the participants. These
standardized tests included the Eating Attitudes Test, Bing Investigatory Test,
Edinburgh and the Hospital Anxiety and Depression Scale, a body dissatisfaction
scale using line drawings, and the Shape- and Weight-Based Self-Esteem Scale.
Both overvaluation of weight and shape and shape- and weight-based self-esteem
were significantly correlated with measures of eating deviations. In addition,
the 159 of the women desired a smaller body shape. However, despite these
associations, the overall degree to which women based their self-esteem on
weight and shape was less than that reported in Western-based studies.
Katsounari (2009) conducted a cross-cultural study to examine two
psychological variables � self-esteem and depression � and their relationship
with eating disturbance in two different cultural contexts, Cyprus and Great
Britain. Participants consisted of 140 randomly selected women, seventy from
Great Britain and seventy from Cyprus, who ranged from nineteen to twenty-five
in age and who were born and raised in Great Britain and Cyprus, respectively.
Selection criteria required the Cyprus females to be able to read English. It
was hypothesized that the women participants of Cyprus would have lower scores
in the self-esteem scale and higher scores in the depression scale, suggesting
higher disturbed eating attitudes than the British sample. Variables were
operationalized using the EAT-40 (Eating Attitudes Test), wherein participants
respond to forty questions on a six-point frequency scale (support to this
measure of assessment is present in both Western and non-Western populations),
the Beck Depression Inventory, which serves as the most prominent and frequently
cited self-report of depression, and the Battle Culture-Free Self-Esteem
Inventory for Adults, which measures perceived self-worth in three subscales:
general self-esteem, personal self-esteem, and social self-esteem; the order of
the questionnaires was counterbalanced to control for order effects.
The analysis of the data gained found that the average self-esteem score
for the British sample (M = 28.7) was higher than the average score reported for
the Cypriot sample (M � 25.620) indicating higher self-esteem for the British
participants. The average depression score for the British sample was lower (M =
5.3) than the Cypriot sample (M = 8.8) indicating that the Cyprus women had
higher depressive tendencies. The average EAT score for the British sample (M =
9.9) was lower than the Cypriot sample (M = 17.1) indicating more disturbed
eating behaviors than the British sample. For both samples, a positive
relationship was found between depression and eating disordered attitudes, which
was found to be significant.
On a more specific note, not many studies have focused on male
participation in studies measuring eating disorders and self-esteem. Even
further, a rare amount has included transsexual subjects, as most of the studies
seem to involve women only. One such study, (Vocks, Stahn, Loenser, & Legenbauer,
2009), attempted to discover whether people with Gender Identity Disorder (GID)
differed from controls of both sexes and people with eating disorders in terms
of the degree of eating and body image disturbance, self-esteem, and depression.
Participants consisted of 356 participants in total, including eighty-eight
self-identified male-to-female (MtF) transsexuals, forty-three female-to-male (FtM)
transsexuals, sixty-two females with an eating disorder, fifty-six male
controls, and 116 female controls. All of the participants completed the Eating
Disorder Examination Questionnaire, Eating Disorder Inventory, Body Checking
Questionnaire, Drive for Muscularity Scale, Rosenberg self-Esteem Scale, and
Beck Depression Inventory.
Results of the study conducted by Vocks (et al., 2009) indicated that MtF
participants showed higher scores on restrained eating, body shape concerns,
drive for thinness, bulimia, body dissatisfaction, and body checking compared to
male controls and even with some variables compared to female controls.
Additionally, FtM displayed a higher degree of restrained eating, weight
concerns, body dissatisfaction and body checking compared to male controls. Even
more, participants with GID showed higher depression scores than did the
controls, though no differences concerning drive for muscularity and self-esteem
were found. One implication of this study was that the participants were
self-identified transsexuals, not diagnosed by the researchers, so therefore it
cannot be known for certainty that each participant fully met the criteria for
GID according to the DSM-IV-TR. This study is important because it speculates
that people with GID might be at a higher risk of eating disorders, therefore
prevention programs should be implemented to help people with GID to avoid
developing an eating disorder.
Another study, conducted by Roberto, Grilo, Masheb, and White (2010),
aimed to compare bulimia nervosa, binge eating, and purging disorder on
clinically significant variables and examine the utility of once versus
twice-weekly diagnostic thresholds for disturbed eating behaviors. Participants
in the study consisted of 234 female community volunteers chosen from a total of
930 respondents who discovered the study through various websites. Participants
were asked to self-report on questionnaires including the Eating Disorder
Examination Questionnaire, the Three Factor Eating Questionnaire, which looks at
cognitive restraining, disinhibition of control over eating, and perceived
hunger, the Questionnaire for Eating and Weight Pattern-Revised, the Beck
Depression Inventory, The Rosenberg Self-Esteem Scale, and self-reported
demographic information, height and current weight were also collected.
The results of this study indicated that bulimia nervosa was a more
severe disorder than binge eating disorder and purging disorder. Additionally,
the three disorders differed significantly in self-reported restraint and
disinhibition; the bulimia nervosa and binge eating disorder groups reported
higher levels of depression than those of the purging disorder. Also, for
bulimia nervosa, participants that engaged in behaviors twice-weekly rather than
once-weekly were more symptomatic in their responses.
In trying to examine the effects of anger, perfectionism, and exercise on
eating pathology among college women, Aruguete, Edman, and Yates (2012)
conducted a study involving 258 students of a California community college who
varied in ethnicity and were unaware of the purpose of the study. The procedure
involved a series of survey questions that measured trait anger and suppressed
anger, eating pathology, exercise commitment, and perfectionism. Trait anger was
measured using the State Trait Anger Expression Inventory and suppressed anger
by the Anger Discomfort Scale. Eating pathology was measured using the Drive for
Thinness Subscale of the Eating Disorder Inventory. Exercise commitment was
evaluated using the Commitment to Exercise scale and the Self-Loathing Subscale
of the Exercise Orientation Questionnaire. Lastly, perfectionism was assessed
using two subscales from the Multidimensional Perfectionism scale: Concern over
Mistakes Subscale and Parental Criticism Subscale.
After performing bivariate correlations to test whether anger,
perfectionism, and exercise commitment would be correlated with eating
pathology, Aruguete (et al., 2012) performed a series of linear regressions to
investigate the effects of anger on perfectionism, exercise commitment, and
eating pathology. The results indicated that exercise and perfectionism (but not
anger) showed significant associations with eating pathology. Additionally, they
found that anger did not independently predict eating pathology, but that trait
anger was negatively associated with exercise commitment and that anger would
independently predict perfectionism. This study supports pervious research,
although one limitation of this study was that it used a convenience sample that
consisted of mostly Asian/Pacific Islanders.
In an attempt to investigate the cross-cultural validity and reliability
of the Chinese Eating Disorder Examination (CEDE) in China, Jun, Jing, Jian,
Hong, Shu Fang, Xiao Yan, and Hsu (2011) conducted an experiment involving
forty-one eating disorder participants and 43 non-eating disorder control
participants of Mainland China. Each group included male and female
participants, and the mean age was 19.86. Though the Eating Disorder Examination
has been supported in prior research to be valid and reliable among Asian
cultures, the researchers sought to examine its reliability in a specific
population of central China after having it translated to Mandarin. The
researchers distributed the CEDE to all participants to evaluate the reliability
and validity in the study population. The reliability indicators were internal
consistency, inter-examiner reliability and test-retest reliability. The
validity indicators were content validity, criterion validity and discrimination
validity. The researchers found the internal consistency, test-retest
reliability, and inter-examiner reliability of the CEDE to be quite high,
indicating that the CEDE has high validity and reliability for the study of
eating disorders in Mainland China. Additionally, they found that the clinical
features of eating disorders among this population are essentially similar to
those of other cultures.
In another study, experimenters (Torres-McGehee, Monsma, Gay, Minton, &
Mady-Foster, 2011) sought to examine the pressures to be thin on female athletes
of appearance-based sports, particularly equestrian athletes. They wanted to
analyze the riding style of the athlete and academic status, along with
perceived body image disturbances. The study was cross-sectional and included
138 volunteer participants of seven universities throughout the United States. A
questionnaire was used to acquire basic and demographic data, such as academic
status and equestrian background, and participants also self-reported their
height, current weight, lowest weight, and ideal weight. Following, the
researchers administered two surveys via email to the participants. The first
was the Eating Attitudes Test, which was used to screen for eating disorder
characteristics and behaviors; the test includes three subscales: dieting,
bulimia, and food preoccupation and oral control. The second, the Figural
Stimuli Survey, was used to asses body disturbance based on perceived and
desired body images; the survey is a scale involving sex-specific body mass
index figural stimuli silhouettes associated with Likert-type ratings of oneself
against nine silhouettes. Chi-square analyses and multivariate analyses of
varies were run to examine the data. Based on the Eating Attitudes Test,
estimated eating disorder prevalence among the participants was 42.0% in the
total sample, 38.5% among English riders, and 48.9% among Western riders. The
experimenters found that no body mass index or silhouette differences were found
across academic status or riding style in eating disorder risk. Also, the
participants perceived their body images as significantly larger than their
actual sizes and wanted to be significantly smaller in everyday clothing and
competitive uniforms.
Recently, descriptive research was conducted by Mond, Peterson, and Hay
(2010) to understand the prior occurrence of regular extreme weight-control
behaviors among women with binge eating disorder. The study involved
twenty-seven women who reported current regular binge eating episodes in the
absence of current regular extreme weight-control behaviors. For each behavior
assessed, participants were first asked whether they had ever engaged in that
behavior, and a positive response to the initial question was followed by a
series or related questions, including whether the behavior was regular. For
this study, �regular� was defined as �on average at least weekly for a period of
three months or more�, and �excessive� as �on average three or more times per
week for a period of three months or more�. Those
who reported the behavior to be a regular occurrence were further asked
questions about the age at which it first occurred and the actual frequency of
the behavior.
Results of this study indicated
that approximately two thirds of participants (65.4%) reported either one or
more purging behaviors at least weekly or one or more non-purging behaviors at a
frequency deemed �excessive� by definition; 38.5% of participants reported
either purging behaviors at least twice weekly or non-purging behaviors five or
more times per week for a period of three months or more. Additionally, five of
the participants had met criteria for bulimia nervosa outlined in the Eating
Disorder Examination, and three of these five participants met criteria for
bulimia nervosa as outlined in the DSM-IV. As for confidence in their
recollections, 38.7% reported to be very confident, 29.0% reported to be
extremely confident, 25.8% reported to be moderately confident, and 6.5%
reported to be a little confident. One implication of this study is that there
may be a considerable overlap between bulimic eating disorders characterized by
binge eating and those characterized by extreme weight-control behaviors.
Previous research has indicated
that body awareness can have an effect on the symptoms of eating disorders. For
instance, in a study conducted by Catalan-Matamoros, Helvik-Skjaerven,
Labajos-Manzanares, Mart�nez-de-Salazar-Arboleas, and S�nchez-Guerrero (2011),
twenty-eight outpatients with eating disorders for less than five years were
treated with body awareness therapy for seven weeks to analyze the feasibility
of improved body awareness in lessening the symptoms of eating disorders. The
participants were randomly assigned into one of two groups: an experimental
group (n=14) and a control group (n=14). The trial consisted of three phases:
the pre-test in which participants from both groups were assessed, the
intervention in which participants in the experimental group received basic body
awareness therapy for seven weeks through twelve sessions, and the post-test in
which participants from both groups were assed at the end. Assessments used in
the pre- and post-tests included the Short Form-36 to assess quality of life,
the Eating Disorder Inventory to
assess the psychological and behavioral common traits in anorexia nervosa and
bulimia, and the Eating Attitude Test-40 to measure symptoms and concerns
characteristic of eating disorders. Data was analyzed to understand the
comparison between the effects produced in the dependent variables of the
experimental and control groups. The results indicated that significant
differences were found in Eating Disorder Inventory and its subscales (mean
difference: 26.3; P=0.015), in Body Attitude Test (mean difference 33.0;
P=0.012), Eating Attitude Test-40 (mean difference: 17.7; P=0.029), and in the
Short Form-36 in the mental health section (mean difference: 13; P=0.002). This
study found that there is some effectiveness of basic body awareness therapy in
improving some symptoms in outpatients with eating disorders; also, that it
heightens the ability to get well, especially in preventing relapses.
In a qualitative research study conducted by Rance, Moller, and Douglas
(2010), seven female counselors who had recovered from eating disorder pasts
participated in semi-structured interviews to examine countertransference
experiences in relation to their body image, weight, and food pathology, their
perceptions about the impact of such experiences and their beliefs about the
effects of their own eating disorder history. The data collection involved
interviews that allowed for the unique, personal experiences of the counselor
while ensuring the areas of interest in the research project were covered. Data
was analyzed by guidelines that focused on themes and connecting features; the
identified themes were ordered in a master table and were: �double-edged
history,� which characterized a common problem faced by the participants,
�emphasis on normality�, which describes a strategy of normalization to overcome
this problem, and the theme of �selective attention�, which illustrates a number
of cognitive and attention strategies employed to enact this solution.
�Double-edged history� illustrated the participants� awareness of both the
benefits and dangers of their eating disorder past. Results of this study shed
light upon an unexplored aspect of the personal and professional experiences of
eating disorder counselors with an eating disorder past. The three themes
illustrate a complex interwoven triad of problem, solution and strategy. The
results suggested that counselors; experienced their eating disorder as a
positive and negative that led them to engage in a number of self-presentational
activities.
Many standard instruments of measure for eating disorders exist, such as
the Eating Disorder Inventory and the Eating Disorder Examination, although
rarely are they examined for applicability among specific populations. In an
attempt to analyze the dimensionality of three versions of the Eating Disorder
Inventory (EDI) in adolescent girls, Garc�a-Grau, Fust�, Mas, G�mez, Bados, and
Salda�a, C (2010) conducted a study involving 738 female adolescents aged
between fourteen and nineteen; the mean age was 15.91 years. The Spanish
adaptations of the Eating Disorder Inventory-1, 2 and 3 were used to assess
psychological, behavioral and affective characteristics related to eating
disorders, although conceptual and structural changes exist between the factors
of the EDI-3 and EDI-2. Goodness of fit and chi-squared tests were employed in
analysis of the data. The results of this study indicated that the dimensional
structure of the three versions of the Eating Disorder Inventory was not clearly
confirmed, at least in this particular sample. However, the shortened version of
the EDI-2 used in this study may be more suitable for use with adolescent girls
in the general population than the original questionnaire.
Sallet, Alvarenga, Ferr�o, de mathis, Torres, Marquess, and
Fleitlich-Bilyk (2010) executed a study to evaluate the prevalence and
associated clinical characteristics of eating disorders in patients with
obsessive-compulsive disorder (OCD) by comparing 815 patients with OCD in a
cross-sectional study. The researchers had three hypotheses: that OCD patients
with comorbid eating disorders would be more frequently women with early onset
of illness and severity of symptoms, have higher prevalence and severity of
contamination obsessions and cleaning compulsions, and show higher rates of
comorbid impulse control orders and body dysmorphic disorder. Assessment was
conducted via structured interviews with mental health professionals with
experience working with OCD and via standardized instruments, such as the
Yale-Brown Obsessive-Compulsive Scale (Y-BOCS), Dimensional Yale-Brown Obsessive
Compulsive Scale (DY-BOCS), Yale Obsessive-Compulsive Disorder Natural history
Questionnaire, Brown Assessment of Beliefs Scale (BABS), Beck Depression and
Anxiety Inventories, and the Clinical Global Impressions Scale (CGI); there were
no self-report assessments.
Results indicated that ninety two
patients (11.3%) presented the following eating disorders: binge-eating
disorders (59, 7.2%), bulimia nervosa (16, 2.0%), or anorexia nervosa (17,
2.1%). Compared to OCD patients without eating disorders, comorbid OCD-eating
disorder patients were more likely to be women with previous mental health
treatment. Additionally, assessment scores were similar within groups; however,
comorbid OCD-eating disorder patients showed higher lifetime predominance of
comorbid conditions, higher anxiety and depression scores, and higher frequency
of suicide attempts than did the OCD group without eating disorders. OCD-eating
disorder patients may be associated with �higher clinical severity.�
Persons with Borderline Personality disorder often struggle with poor
self-esteem. In a unique study conducted by Zanarini, Reichman, Frakenburg,
Reich, and Fitzmaurice (2010), researchers attempt to describe the longitudinal
course of eating disorders in patients with borderline personality disorder. The
Structured Clinical Interview for DSM-III-R axis I Disorders (SCID-1), the
Revised Diagnostic Interview for Borderlines (DIB-R) and the Diagnostic
Interview for DSM-III-R Personality Disorders (DIPD-R) were administered to 290
borderline inpatients and seventy-two participants with other axis II disorders
during their index admission and at five contiguous two-year follow-up periods.
Participants had a mean GAF score of
39.8, indicating major impairment in several areas. Results of the study
indicated that the prevalence of anorexia, bulimia and eating disorder not
otherwise specified declined significantly over time for those in both study
groups; however, the prevalence of eating disorder not otherwise specified
remained significantly higher among borderline patients. Over 90% of borderline
patients meeting criteria for one of the eating disorders experienced a stable
remission by the time of the ten-year follow-up, although diagnostic migration
was common. Additionally, both recurrences and new onsets of eating disorder not
otherwise specified were more common among borderline patients than recurrences
and new onsets of anorexia nervosa and bulimia.
In a study assessing the quality of life, course and predictors of
outcomes in community women with eating disorders not otherwise specified and
common eating disorders, researchers (Hays, Buttner, Mond, Paxton, Rodgers,
Quirk, & Darby, 2010) sought to describe the functional and symptomatic outcome
these women. The researchers investigated the two-year course and supposed
predictors of outcome of eighty-seven young community women with common eating
disorders following a health literacy (informational) intervention; the health
literacy intervention was provided randomly to half participants at baseline and
half at one year. The instruments of assessment included the Eating Disorder
Examination, the Short Form-12 Health Status Questionnaire, Kessler-10 for
general psychiatric symptoms, and the Defense Style Questionnaire. During the
follow-up assessments, researchers measured alcohol and substance misuse and
distributed the Life Events Checklist to indicate if the participant has
experienced a variety of life events over the last twelve months. Results of
multiple linear regression analyses indicated that eating disorder
psychopathology remained high and mental health quality of life remained poor.
For multivariate models, a higher baseline level of immature defense style
significantly predicted higher levels of eating disorder symptoms as well as
poorer mental health quality of life. Also, in line with the research conducted
by de la Rie (et al., 2005), women with common eating disorders followed to two
years continued to be highly symptomatic and have poor quality of life.
A similar study, conducted by Mu�oz, Quintana, Hayas, Aguirre, Padiema,
and Gonz�lez-Torres (2009) aimed to evaluate and compare the quality of life in
patients with eating disorders and general population, using the
disease-specific Health-Related Quality of Life for Eating Disorders (HeRQoLED)
questionnaire. Participants consisted of 358 patients with eating disorders who,
upon inclusion into the study, were sent three measurement instruments: the
HeRQoLED, the Eating Attitudes Test (EAT-26) and the Short Form-12. Each patient
took part in psychopharmacologic and psychotherapeutic treatment programs, and
after one year of treatment and follow-up, the three questionnaires were sent
again to the participants. Univariate analysis was performed to determine which
variables were predictive of change in each of the HeRQoLED domains after one
year of treatment, and general linear models were performed to establish
variables for the multivariate analysis. Results indicated that patients with
anorexia nervosa had higher baseline scores (indicating worse perception of
quality of life on the HeRQoLED questionnaire and experienced smaller
improvements that patients with other eating disorder diagnoses after one year
of treatment. Body-mass index and EAT-26 scores were associated with changes in
quality of life. Short Form-12 scores showed significant improvement in the
physical component but not in mental health. Additionally, quality of life in
patients with eating disorders improved after one year of treatment, though it
did not reach the values of the general population.
In the current study, the researcher wanted to understand the
relationship and interactions between self-esteem, gender, and eating disorders.
The objective was to replicate similar studies to determine if having low levels
of self-esteem or self-worth contributed to the development of eating disorders
and whether or not gender impacted the prevalence of eating disorders. It was
hypothesized that students with high self-esteem were less likely to suffer from
eating disorders, including binge eating, bulimia nervosa, and anorexia nervosa.
The independent variable is self-esteem, which was measured by asking the
student participants questions regarding their self-worth and feelings towards
themselves. The dependent variables are the eating disorders: bulimia nervosa,
anorexia nervosa and binge eating. Another hypothesis was that women are more
likely than men to suffer from eating disorders, where gender is the independent
variable, and suffering from an eating disorder is the dependent variable.
Eating disorders were evaluated by asking the student participants questions
about their eating, exercising, dietary habits, and experience with eating
disorders. Body type was also evaluated by asking the participants to select one
of the given categories on the survey for themselves and for members of their
immediate family; the categories consist of different body shapes such as
underweight, average, or overweight. The survey consists of fifty-three
questions in total, including demographic information, Likert scales, the
categorical response of body type, and yes or no questions. It was hypothesized
that students that have or have had an eating disorder are more likely to report
low levels of self-esteem and that women are more likely than men to suffer from
eating disorder.
Method
Participants
A sample of 100 college students
was randomly selected from a small, private, liberal arts college in the midwest.
There were 45 males, 52 females, and 3 participants that did not report a
gender. Participants included 21 freshmen, 29 sophomores, 23 juniors, 17
seniors, 2 students in their fifth year or more, and 8 participants that did not
report their year in school. Participation was a convenience sample and
participants had the choice to withdraw at any point in time. The classes in
which the surveys were distributed were: Introduction to Psychology, Victorian
English Literature, Introduction to Ethics, and Introductory Biology.
Materials
The survey was designed by the
researcher with questions adapted from the Index of Self-Esteem (ISE) and
consisted of a questionnaire using 53 close-ended questions, presented using
constancy. The survey included questions about eating habits, the participants�
body shape, how the participants feel about themselves, and other items relating
to experience with eating disorders. Other questions included demographic
information, such as gender, year in school, and body type. All 100 surveys that
were distributed were returned, which may aid in the validity of this research.
Procedure
The surveys were distributed in classrooms based on a convenience sample.
Participants were asked to complete every question of the survey and were
instructed to ask the researcher if there were any questions. The questions
referring to self-esteem and dietary habits were designed to measure how the
participants feel about themselves (their perceived self-esteem) and whether or
not their eating pathology predisposed them to weight concern or an eating
disorder. The eating disorder items served to determine outright whether or not
the participants had prior exposure to eating disorders either through their
friends or personal experience. Surveys were completely anonymous; participants
signed their initials and dated the consent form, which they handed in
separately from the survey (see appendix). The survey was field tested in a
classroom of psychology majors studying experimental psychology, revised, and
was submitted to McKendree University�s Institutional Review Board along with
the purpose of research, hypotheses, and an agreement to abide by ethical
principles of research with human participants. It received Institutional Review
Board approval, valid for one year until March 8, 2013, exempt from IRB review
for its anonymity and data from consenting adult college students. Ethical
guidelines outlined by APA were followed. Statistical tests conducted to analyze
data include one-way ANOVAs, independent samples t-tests, and correlation
analyses to determine results.
Results
Figure
1
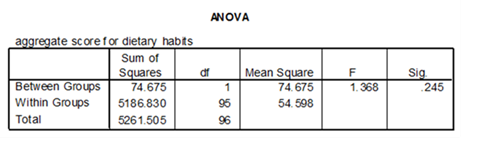
Figure 2
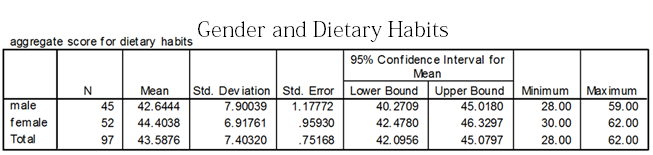
Figures 1 and 2 show the results
in using a one-way ANOVA to test whether gender has an impact on dietary habits.
Results indicated no significant difference in dietary habits based on gender, F
(1, 95) = 1.368, p = 0.245. Statistically, females were no more likely than
males to endorse healthier eating patterns.
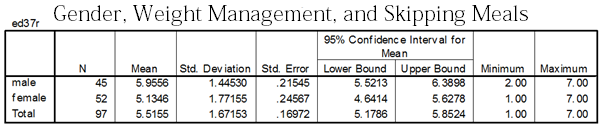
Figure 3
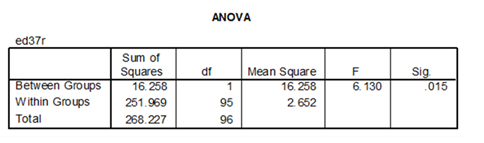
Figure 4
Figures 3 and 4 show the results
in using a one-way ANOVA to test whether gender influences meal skipping in an
effort engage in weight management. Results indicated a significant difference
in meal skipping to engage in weight management based on gender, F (1, 95) =
6.130, p = 0.015. It was found that more often than males, females reported that
they skip meals to engage in weight management.
 Figure
5
Figure
5
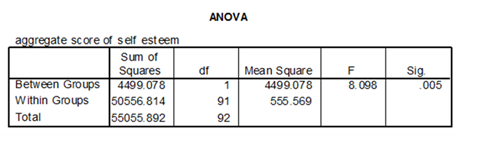
Figure 6
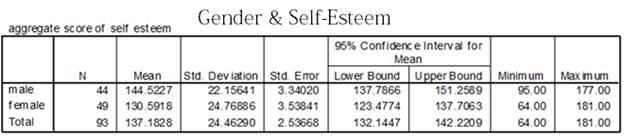
Figures 5 and 6 show the results
in using a one-way ANOVA to test whether gender has an impact on a person�s
self-esteem. Results indicated a significant difference in self-esteem based on
gender, F (1, 91) = 8.098, p = 0.005. It was found that females reported lower
levels of self-esteem than did males.
 Figure
7
Figure
7
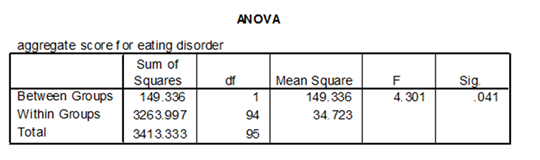
Figure 8
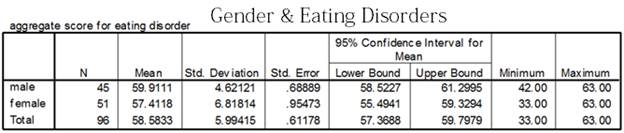
Figures 7 and 8 show the results
in testing the hypothesis that gender impacts an individual�s experience with
eating disorders by using a one-way ANOVA. Results indicated a significant
difference in experience with eating disorders based on gender, F (1, 94) =
4.301, p = 0.041. Statistically, females were more likely than males to report
experience with eating disorders, including bulimia nervosa, anorexia nervosa,
or binge eating.
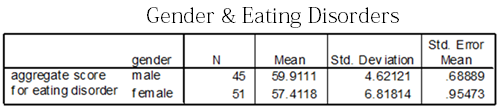
Figure 9
 Figure
10
Figure
10
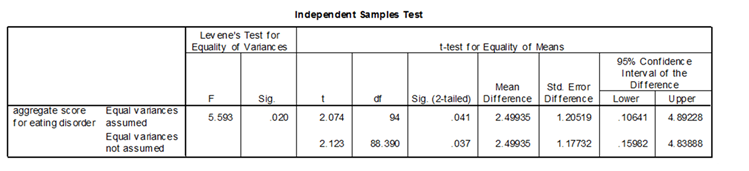
Figures 9 and 10 show the results in again testing the hypothesis that
gender impacts an individual�s experience with eating disorders by using an
independent samples T-test. The independent samples T-test analysis comparing
scores for males and females on eating disorders indicated that female scores (M
= 59.9, SD = 4.62) differed significantly from male scores (M = 57.4, SD =
6.82), t(94) = 2.074, p = 0.0205.
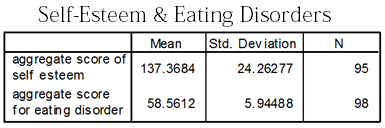
Figure 11
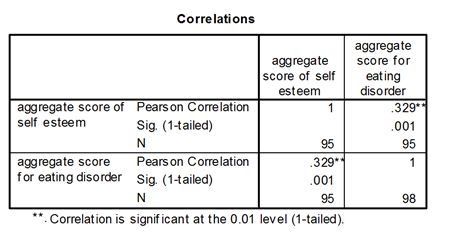
Figure 12
Figures 11 and 12 show the results in testing the hypothesis that
self-esteem is directly related to the development of an eating disorder by
using a correlation analysis. A Pearson�s Bivariate Correlation found a
significant relationship between self-esteem and eating disorders, (r = 0.329, p
= 0.001). It was found that participants who reported higher self-esteem also
reported less experience with eating disorders.
Discussion
The current research study can relate to a significant amount of other
studies that have sought to examine the interactions between self-esteem,
gender, and eating disorders. This study stands out from the others in that it
sought to examine the correlation between gender and self-esteem, gender and
eating disorders, and self-esteem and eating disorders. Though no solution was
found through the current study to diminish the prevalence of eating disorders,
awareness of the correlations between self-esteem, gender, and eating disorders
may prompt further research in finding how to improve self-esteem and minimize
eating disorders among college students, especially females.
While intriguing results,
implications, and correlations were found, limitations were present as well. One
limiting factor that may have affected the results was the small, convenience
sample size of participants, which did not allow for a full representation of
all college students. A larger sample size across a wider spread of campuses
would provide higher validity than did the current study. Additionally, the
survey should have included further demographic information, such as age, for
descriptive statistical purposes, and questions about the standard of body image
regarding gender.
The first prediction was that students with high self-esteem are less
likely to suffer from eating disorders, including binge eating, bulimia nervosa,
and anorexia nervosa. The results showed that there was a statistically
significant difference in that those who reported higher self-esteem also
reported less experience with eating disorders. This could be because those with
a higher sense of self-worth may not have as many body image issues and may
endorse a healthier eating pathology. Results of previous research studies (e.g.
Ross & Wade, 2004) indicated that self-esteem and weight shape concern together
accounted for about one-third of the variance in uncontrolled eating.
Another hypothesis that was presented prior to research was that women
are more likely than men to suffer from eating disorders. The results indicated
a statistically significant relationship between gender and eating disorders,
where females rated themselves lower for self-esteem and were more likely to
report experience with an eating disorder than did males. This could be because
society and the media instill a higher standard of body shape and image in
females at a young age than in males, which becomes impressed in how they view
themselves as adults. Many females struggle with body image expectations
throughout their lifetime, which may lead to the development of specific eating
and exercise pathologies.
It is worth noting that although both hypotheses were supported, results
indicated no significant difference in dietary habits based on gender. The
significant results of the current study may lead to new directions for this
research in the future. Perhaps further studies will begin to explore the impact
of gender and body expectations on self-esteem and eating disorders in the
college population. Subsequent research could lead to a greater understanding of
the factors that influence gender-specific body expectations, self-esteem, and
eating disorders; this could result in efforts to improve self-esteem and
minimize eating disorders among college students, especially those that are
female. There are many dangers related to eating disorders and low self-esteem,
especially during college, when students seem to be more vulnerable and critical
of themselves. The current study is intriguing and can most certainly add
validity to previous research and also advance towards new findings in the
future.
References
Aruguete, M.
S., Edman, J. L., & Yates, A. (2012). The Relationship between Anger and other
Correlates of Eating Disorders in Women. North American Journal Of Psychology,
14(1), 139-148.
Bardone-Cone,
A. M., Schaefer, L. M., Maldonado, C. R., Fitzsimmons, E. E., Harnby, M. B.,
Lawson, M. A., & � Smith, R. (2010). Aspects of Self-Concept and Eating Disorder
Recovery: What Does the Sense of Self Look Like When an Individual Recovers from
an Eating Disorder?. Journal of Social & Clinical Psychology, 29(7), 821-846.
Catalan-Matamoros, D., Helvik-Skjaerven, L., Labajos-Manzanares, M., Mart�nez-de-Salazar-Arboleas, A., & S�nchez-Guerrero, E. (2011). A pilot study on the effect of Basic Body Awareness Therapy in patients with eating disorders: a randomized controlled trial. Clinical Rehabilitation, 25(7), 617-626.
De la Rie, S. M., Noordenbos, G., & van Furth, E. F. (2005). Quality of Life and Eating Disorders. Quality of Life Research, Vol. 14.
Garc�a-Grau,
E., Fust�, A., Mas, N., G�mez, J., Bados, A., & Salda�a, C. (2010).
Dimensionality of three versions of the eating disorder inventory in adolescent
girls. European Eating Disorders Review, 18(4), 318-327.
Green, M. A., Scott, N. A., Cross, S. E., Liao, K., Hallengren, J. J., Davids, C. M., & ... Jepson, A. J. (2009). Eating disorder behaviors and depression: a minimal relationship beyond social comparison, self-esteem, and body dissatisfaction. Journal of Clinical Psychology, 65(9), 989-999.
Hay, P.,
Buttner, P., Mond, J., Paxton, S. J., Rodgers, B., Quirk, F., & Darby, A.
(2010). Quality of life, course and predictors of outcomes in community women
with EDNOS and common eating disorders. European Eating Disorders Review, 18(4),
281-295.
Hesse-Biber, S., Marino, M., & Watts-Roy, D. (1999). A Longitudinal Study of Eating Disorders among College Women: Factors That Influence Recovery. Gender and Society, Vol. 13.
Jun, T., Jing, S., Jian, W., Hong, Z., Shu Fang, Z., Xiao Yan, W., & Hsu, L. (2011). Validity and reliability of the Chinese language version of the eating disorder examination (CEDE) in mainland China: Implications for the identity and nosology of the eating disorders. International Journal Of Eating Disorders, 44(1), 76-80.
Katsounari, I. (2009). Self-esteem, depression and eating disordered attitudes: A cross-cultural comparison between Cypriot and British young women. European Eating Disorders Review, 17(6), 455-461.
Mond, J. M., Peterson, C. B., & Hay, P. J. (2010). Prior use of extreme weight-control behaviors in a community sample of women with binge eating disorder or subthreshold binge eating disorder: A descriptive study. International Journal Of Eating Disorders, 43(5), 440-446.
Mu�oz, P. P., Quintana, J. M., Hayas, C., Aguirre, U. U., Padierna, A. A., & Gonz�lez-Torres, M. A. (2009). Assessment of the impact of eating disorders on quality of life using the disease-specific, Health-Related Quality of Life for Eating Disorders (HeRQoLED) questionnaire. Quality Of Life Research, 18(9), 1137-1146.
Rance, N. M., Moller, N. P., & Douglas, B. A. (2010). Eating Disorder Counsellors With Eating Disorder Histories: A Story of Being 'Normal'. Eating Disorders, 18(5), 377-392.
Roberto, C. A., Grilo, C. M., Masheb, R. M., & White, M. A. (2010). Binge eating, purging, or both: Eating disorder psychopathology findings from an internet community survey. International Journal Of Eating Disorders, 43(8), 724-731.
Ross, M., & Wade, T. D. (2004). Shape and weight concern and self-esteem as mediators of externalized self-perception, dietary restraint and uncontrolled eating. European Eating Disorders Review, 12(2), 129-136.
Sallet, P. C., de Alvarenga, P., Ferr�o, Y., de Mathis, M., Torres, A. R., Marques, A., & ... Fleitlich-Bilyk, B. (2010). Eating disorders in patients with obsessive�compulsive disorder: Prevalence and clinical correlates. International Journal Of Eating Disorders, 43(4), 315-325.
Tchanturia, K., Troop, N. A., & Katzman, M. (2002). Same pie, different portions: shape and weight-based self-esteem and eating disorder symptoms in a Georgian sample. European Eating Disorders Review, 10(2), 110-119.
Torres-McGehee,
T. M., Monsma, E. V., Gay, J. L., Minton, D. M., & Mady-Foster, A. N. (2011).
Prevalence of Eating Disorder Risk and Body Image Distortion Among National
Collegiate Athletic Association Division I Varsity Equestrian Athletes. Journal
Of Athletic Training, 46(4), 431-437.
Vocks, S., Stahn, C., Loenser, K., & Legenbauer, T. (2009). Eating and Body Image Disturbances in Male-to-Female and Female-to-Male Transsexuals. Archives Of Sexual Behavior, 38(3), 364-377.
Zanarini, M.
C., Reichman, C. A., Frankenburg, F. R., Reich, D., & Fitzmaurice, G. (2010).
The course of eating disorders in patients with borderline personality disorder:
A 10-year follow-up study. International Journal Of Eating Disorders, 43(3),
226-232.
APPENDIX A
Read this consent form. If you have
any questions ask the experimenter and
She will answer your questions.
�I have read the statement below and have been fully advised of the procedures
to be used in this project. I have
been given sufficient opportunity to ask any questions I had concerning the
procedures and possible risks involved.
I understand the potential risks involved and I assume them voluntarily.�
Please sign your initials, detach below the dotted line, and continue with the
survey.
Sign your initials here_________________
Date__________
----------------------------------------------------------------------------------------------------------------------------------------
The McKendree University Psychology Department supports the practice of
protection for human participants participating in research and related
activities. The following
information is provided so that you can decide whether you wish to participate
in the present study. Your
participation in this study is completely voluntary.
You should be aware that even if you agree to participate, you are free
to withdraw at any time, and that if you do withdraw from the study, your
grade in this class will not be affected in any way.
This survey is being conducted to assist the researcher in fulfilling
a partial requirement for PSY 496W.
You must be over 18 years of age to participate in the survey.
It should not take more than 10 minutes for you to complete and will be
completely anonymous and confidential.
If you should have any other questions, don�t hesitate to contact me,
Cassandra Fremder, 618-830-7052 or at cbfremder@mckendree.edu, or Dr. Bosse,
618-537-6882 or at
mbosse@mckendree.edu.
Some of the questions in the survey may confront sensitive topics.
If answering any of these questions causes you problems or concerns,
please contact one of our campus psychologists, Bob Clipper or Amy Champion-Stahlman,
at 537-6503.
Rev. 3/31/09
APPENDIX B
STUDENT SURVEY
Gender: Male _____
or
Female ���_____
Year in School:
Freshman
Sophomore
Junior
Senior
5th Year or more
1. Please indicate your family�s body builds with an X. (Use additional X�s for
multiple siblings.)
Underweight
Average
Overweight
Mother:
_____
_____
_____
Father:
_____
_____
_____
Sister(s):
_____
_____
_____
Brother(s):
_____
_____
_____
Self:
_____
_____
_____
Please respond to numbers 2- 45 based on the following scale:
1 - Never
2 - Almost Never
3 - Rarely
4 - Sometimes
5 - Frequently
6 - Almost Always
7 � Always
(Please circle only one.)
2. I snack with healthy food.
1
2
3
4
5
6
7
Never
Almost Never
Rarely
Sometimes
Frequently
Almost Always
Always
3. I count calories.
1
2
3
4
5
6
7
4. I rely on other people to feel good about myself.
1
2
3
4
5
6
7
5. I exercise on a regular basis.
1
2
3
4
5
6
7
6. I am on a diet/dieting.
1
2
3
4
5
6
7
7. I feel good about myself.
1
2
3
4
5
6
7
8. I eat a lot of vegetables.
1
2
3
4
5
6
7
9. I depend on others for attention.
1
2
3
4
5
6
7
Never
Almost Never
Rarely
Sometimes
Frequently
Almost Always
Always
10. I worry about my appearance.
1
2
3
4
5
6
7
11. I eat a lot of junk food.
1
2
3
4
5
6
7
12. I eat breakfast.
1
2
3
4
5
6
7
13. I eat at least three balanced meals a day.
1
2
3
4
5
6
7
14. I worry about my weight.
1
2
3
4
5
6
7
15. I feel as if I am in control of my decisions and actions.
1
2
3
4
5
6
7
16. I feel healthy.
1
2
3
4
5
6
7
17. I feel dependent on others.
1
2
3
4
5
6
7
18. I think that I am a dull person.
1
2
3
4
5
6
7
19. I like my body.
1
2
3
4
5
6
7
20. I am concerned if other people like my body.
1
2
3
4
5
6
7
21. I drink beer or alcohol.
1
2
3
4
5
6
7
22. I eat a lot of fruit.
1
2
3
4
5
6
7
23. I consume drinks high in sugar.
1
2
3
4
5
6
7
24. I smoke.
1
2
3
4
5
6
7
Never
Almost Never
Rarely
Sometimes
Frequently
Almost Always
Always
25. I feel that people would not like me if they really knew me well.
1
2
3
4
5
6
7
26. When I am with other people, I feel they are glad I am with them.
1
2
3
4
5
6
7
27. I feel that I am a very competent person.
1
2
3
4
5
6
7
28. I think I make a good impression on others.
1
2
3
4
5
6
7
29. I feel that I need more self-confidence.
1
2
3
4
5
6
7
30. I stare into mirrors and windows to see what I look like.
1
2
3
4
5
6
7
31. I believe that other people are staring at me when I walk into a room.
1
2
3
4
5
6
7
32. I would say I am obsessed with what my body looks like.
1
2
3
4
5
6
7
33. I have confidence in myself.
1
2
3
4
5
6
7
34. I am confident about my body.
1
2
3
4
5
6
7
35. I have high self-esteem.
1
2
3
4
5
6
7
36. I like what I see when I am looking in a mirror.
1
2
3
4
5
6
7
37. I have skipped meals before to engage in weight management.
1
2
3
4
5
6
7
38. I feel that others have more fun than I do.
1
2
3
4
5
6
7
39. I think I have a good sense of humor.
1
2
3
4
5
6
7
Never
Almost Never
Rarely
Sometimes
Frequently
Almost Always
Always
40. I feel very self-conscious when I am with strangers.
1
2
3
4
5
6
7
41. I am afraid I will appear foolish to others.
1
2
3
4
5
6
7
42. I think my friends find me interesting.
1
2
3
4
5
6
7
43. I binge eat.
1
2
3
4
5
6
7
44. If so, I feel guilty after binge eating.
1
2
3
4
5
6
7
45. I engage in purging (throwing up) after meals to help with weight
management.
1
2
3
4
5
6
7
Please respond to numbers 46- 51 based on the following scale:
1 - Strongly Disagree
2 - Disagree
3 - Slightly Disagree
4 - Neither Agree nor Disagree
5 - Slightly Agree
6 - Agree
7 - Strongly Agree
(Please circle only one.)
46. I think I may have a problem with binge eating.
1
2
3
4
5
6
7
Strongly Disagree
Strongly Agree
47. I think I used to have a problem
with binge eating.
1
2
3
4
5
6
7
48. I think I may have a problem with anorexia nervosa.
1
2
3
4
5
6
7
49. I think I used to have a problem with anorexia nervosa.
1
2
3
4
5
6
7
50. I think I may have a problem with bulimia nervosa.
1
2
3
4
5
6
7
Strongly Disagree
Strongly Agree
51. I think I used to have a problem with bulimia nervosa.
1
2
3
4
5
6
7
Please circle one.
52. I have/had friends with bulimia nervosa.
YES
NO
53. I have/had friends with anorexia nervosa.
YES
NO
THANK YOU FOR COMPLETING THIS SURVEY.
Survey questions adapted from the Index of Self-Esteem (ISE)